AMH in Ovarian Physiology
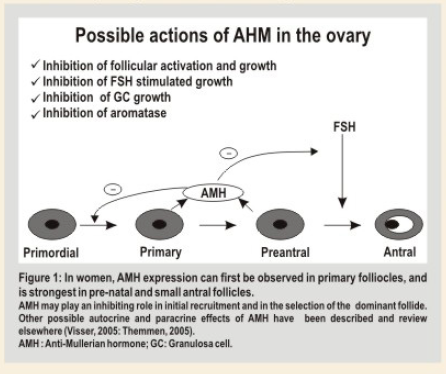
AMH is produced by granulosa cells from preantral and antral follicles, AMH is expressed on follicles that have undergone recruitment from primordial follicles pool but have not been selected for dominance by the action of FSH. In human this occurs in antral follicles of size 4-6 mm. AMH is not expressed in primordial follicles, atreticfollicles and theca cells.
The main physiological role of AMH in ovary seems to be limited to inhibition of the early stages of follicular development (Figure 1). Several studies have confirmed the concept that in the absence of AMH, primordial follicles are recruited at a faster rate, resulting in premature exhaustion of primordial follicle pool. In vitro studies have shown that AMH inhibits FSH dependent follicular growth and regulates ovarian steroidogenesis by decreasing expression of aromatase on granulosa cells thus decreasing estradiol production. AMH reduces LH receptor on granulosa cells stimulated by FSH.
Factors Modulating AIVIH Levels In Women In women
AMH levels are almost undetectable at birth with a subtle increase within first 2 or 4 years of age, after that AMH appears to be stable until adulthood but found to decrease as a sign of follicular reserve exhaustion becoming undetectable at menopause.
AMH levels seem to be unmodified under conditions in which endogenous gonadotropins release is substantially diminished such as during pregnancy, GnRH agonist treatment and short term oral contraceptive administration, indi.ting that non cyclic FSH independent ovarian activity persist, even when pituitary FSH is suppressed.
AMH levels in obese women may be lower for physiological reasons related to obesity itself and may not necessarily indicative of impaired ovarian reserve. Other factors related to reducedAMH levels are smoking, alcohol use and certain race or ethnicity.
AMH in Ovarian Reserve Testing
The ovarian reserve, constituted by the size of ovarian follicles pool and the quality of oocytes therein, declines which increasing age, resulting in the decrease of a woman, reproductive function.
For women who want to become pregnant by means of assisted reproduction technique (ART), it is important to offer counseling about the optimal balance between benefit and risk. Since these out comes are highly dependant on ovarian reserve, much efforts have been put in identifying good clinical markers of ovarian reserve regarding individuals prognosis for success and to design appropriate stimulation protocols.
An ideal ovarian reserve test should permit identification of women who have a chance of pregnancy after IVF close to zero as a consequence of an extremely reduced ovarian reserve. The exclusion of these couples from ART could effectively reduce costs for the health system. Moreover unnecessary medical treatments, stress and disappointment could be avoided. The possible aims of ovarian reserve testing in the IVF setting are:
i. Tocounsel the patients about the risk benefit for treatment.
ii. To reduce the cost by denying treatment to bad prognosis couples.
iii. To individualize treatment strategy.
To assess an individual’s ovarian reserve, early follicular phase serum levels of FSH, inhibin B and estradiol (E2) have been measured. Inhibin B and E2 are produced by early antral follicles in response to FSH, and contribute to classical feedback loop of the pituitary•gonadal axis to suppress FSH secretion. With the decline of follicle pool, serum level of inhibin B & E2 decreases & subsequently FSH rises. Because these factors are part of a feedback system, their levels are not independent of each other. Furthermore changes in serum level of FSH, inhibin B and E2 occurs late in reproductive ageing process. So far, assessment of number of antral follicles by USG, the antral follicles counts (AFC) best predicts the quantitative aspect of ovarian reserve. However, AFC at times is technically challenging and highly operator dependent. Therefore, a serum marker that reflects the number of follicles that have made the transition from the primordial pool into growing follicle pool, and that is not controlled by gonadotropins, would benefit both patients & clinicians.
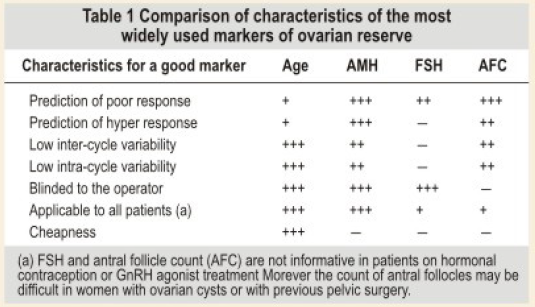
Recently, AMH has been proposed as an ideal test for ovarian reserve testing (Table 1) due to the following characteristics:
1. Decreases continually during the fertile life.
2. Not influenced bygonadotropin feedback mechanism.
3. AMH level shows very low inter and intracycle variability thus can be measured independent of the day of cycle.
4. Bestcorrelating marker withAFC.
Significance of lowAMH levels before IVF
For women with low AMH levels either cycle cancellation or poor response may be anticipated. Her. couple need to accept protract. treatment programs and should be inform. that not every cycle may result in embryo transfer and that it is highly probable that chance of suc.ss may be reduced. Cut -off values of 0.7 — 0.75 ng/ml has been proposed by several groups for the identificetion of poor responders, by this cut off 75% of poor responder are correctly identified.
Significance of NormalAMH levels before IVF:
Wornen with normal AMH levels are most probably normal responders and good prognosis may be anticipated.
Significance of high AMH levels before IVF:
Women with high AMH levels are considered to be at risk for hyperresponse and OHSS. Hence these wornen should be informed about the risk and may really benefit from individualization of the treatment. Indeed a low FSH starting dose followed by the use of GnRH antagonists have been shown to reduce the incidence of OHSS.
AMH AS A MARKER OF OVARIAN AGING
Quantitative aspect of ovarian aging is reflected by a decline in size of the primordial follicle pool. Direct measurement of this pool is impossible. However, the number of Primordial follicles is directly reflected by number of growing follicles. Sin. AMH is secreted by growing follicles up to selection, it seerns to be a promising cendidate. Moreover changes in AMH levels occur relatively early in the sequence of events associated with ovarian aging. Substantially elevated serum levels of FSH are not found until cycles have become irregular. Therefore, a marker that already shows a considerable change when cyclicity is still norrnal would better identify women with declining fertility.
Measurement of AMH to assess ovarian age may be of considerable interest for wornen in general since a considerable proportion of subferility is due to postponement of child bearing. Measurement of ovarian reserve may provide insight into the number of fertile year’s women has left.
AMH as A Marker for Ovarian Pathophysiology
Besides being a marker for diminishing follicle pool serum AMH level cen a. serve as a marker in ovarian pathophysiology, such as polycystic ovary syndrome (PCOS), in which the antral follicle pool is enlarged. In PCOS women, the Iwo to threefold increase in number of growing follicles is reflected by two to three fold increases in serum AMH level. In PCOS, follicular excess is mainly ceused by an increase in small antral follicles up to 2-5 mm size. Interestingly, in follicles beyond this stage AMH expression decreases. Therefore, it is not surprising that serum AMH levels positively correlate with number of 2-5 mm, but not 6-9 mm follicles in PCOS women. The finding thatAMH level is also increased in the follicular fluid of PCOS women suggests that an increase in serum AMH may also result from increased AMH production per follicle. Some of the studies have indicated that PCOS women reach menopause atan older age. The ovarian ageing process in PCOS women may have been slowed down. possibly due to suppre.ed prirnordial follicle outgrowth by the high levels of AMH observed in the. women. AMH levels appear to be related to severity of the syndrome since levels have been observ. to be higher in insulin resistant PCOS women than in patients with normal insulin sensitivity. Similarly AMH is higher in amenorrheic compared with oligomenorrheicwomen with PCOS.
Conclusion
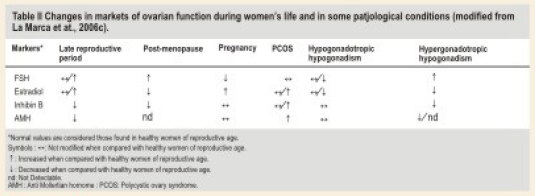
The currently available data indicate that serum AMH levels decrease with age in premenopausal women. Assessment of ovarian reserve is particularly important in IVF clinic. A serum level of AMH strongly correlates with antral follicle count and reflect the size of primordial follicle pool thus may be useful as a predictor of ovarian responsiveness. The changes in AMH levels in several physiological and pathological conditions are reported in Table 2.
AMH may permit the identification of both the extremes of ovarian stimulation: a possible role for its measurement may be in the individualization of treatment strategies. Furthermore, AMH measurement in combination with other tests of ovarian reserve (antral follicle count, FSH, estradiol and Inhibin B levels) can assist women in making more informed family planning decisions based on their own individual risk of experiencing premature loss of ovarian reserve.